A dysplastic or atypical nevus is a benign (noncancerous) mole that is not a malignant melanoma (cancerous), but has an unusual appearance and/or microscopic features. Dysplastic moles usually appear in individuals during their 20s and can be found anywhere on the body, such as the scalp, but are more common on sun-exposed areas, such as the trunk and extremities. Dysplastic moles have a higher tendency to develop into malignant melanoma than benign moles.
What does a dysplastic mole look like?
Dysplastic moles can vary in appearance. A dysplastic mole often displays minor asymmetry or lack of mirror-image. One half does not match the other half in size, shape, color, or thickness. The edges of a dysplastic mole can be poorly defined but are not scalloped or notched as seen in malignant melanoma. Dysplastic moles may have multiple colors, including shades of brown, black, and pink; however, the coloration is fairly uniform. Dysplastic moles tend to be larger than benign moles, ranging from 3 to 15 millimeters [Figure 1]. Dysplastic moles tend to remain the same, while malignant melanomas continue to grow and change.
Why is it important to know about dysplastic moles?
A dysplastic mole can sometimes develop into skin cancer. Skin cancer arising from a dysplastic mole is malignant melanoma, which is a very dangerous type of skin cancer that can be fatal if not treated early. The best way to survive malignant melanoma is to diagnose and treat it early. The best way to diagnose it early is to perform a weekly skin self-exam and to be suspicious about any new mole, changing mole, or mole that looks different or unusual from those in the surrounding area. If any mole looks suspicious, you should report it immediately to your dermatologist.
Malignant melanoma can arise from a dysplastic mole, a previously normal mole, or from normal-appearing skin. Therefore, it is important to be familiar with all of your moles and to remember if a mole was there or not and what it looks like. Your weekly skin self-exam will help you familiarize and remember what your moles look like. If you see any new mole, changing mole, or a mole that looks different or unusual from those in the surrounding area, report it immediately to your dermatologist. Malignant melanoma can develop tomorrow or any time in the future, so make sure you perform a weekly skin self-exam throughout your life.

Figure 01
Relationship between dysplastic moles and malignant melanoma
- A patient with a few dysplastic moles who does not have a personal or family history of malignant melanoma is at a slightly higher risk than the general population for developing malignant melanoma
- The presence of multiple dysplastic moles may increase the risk of developing a malignant melanoma; this risk increases with the number of dysplastic moles
- A patient with dysplastic moles who has a personal or family history of malignant melanoma is at a higher risk for developing malignant melanoma
- A patient with multiple dysplastic moles may have dysplastic nevus syndrome (DNS), and is at an increased risk for developing malignant melanoma, especially if a relative had malignant melanoma
- DNS, also known as familial atypical mole-malignant melanoma syndrome (FAMMM), is a diagnosis given to individuals who meet the following criteria:
- Have a first-degree relative (such as a parent, sibling, or child) or a second-degree relative (such as a grandparent, grandchild, aunt, or uncle) who has had malignant melanoma
- Have a large number of moles (more than 50), many of which are atypical or dysplatic moles
- Have moles that demonstrate atypical microscopic features on biopsy
Some people and families who meet these criteria may be carriers of a genetic mutation that predisposes them to malignant melanoma. Genetic testing is not yet routinely performed but should be considered in certain instances. Some families who carry the genetic mutation can also be predisposed to developing pancreatic cancer.
Risk factors
Anyone can get malignant melanoma, but there are certain risk factors that make some individuals more susceptible to malignant melanoma than others. Risk factors increase your susceptibility to malignant melanoma; however, they do not mean you will develop malignant melanoma.
Risk factors for malignant melanoma include
- Personal and family (genetic) history
- Fair skin with red hair and blue eyes
- Male over 50 years old
- Increased number of moles: having more than 50 moles increases the risk of malignant melanoma
- Having atypical or dysplastic moles
- Personal history of malignant melanoma
- Family history of malignant melanoma, such as a parent, brother, sister, aunt, or uncle
- Environmental exposure
- Excessive long-term sun and ultraviolet light exposure
- Fair skin and having grown up in a southern region
- Frequent exposure to outside work or recreation
- History of multiple sunburns
- Freckles
- Use of an indoor tanning lamp or bed
- Medical condition that suppresses the immune system, such as AIDS or medications that organ transplant recipients take to suppress their immune system
- Excessive long-term sun and ultraviolet light exposure
How are dysplastic moles diagnosed?
Inspection of your skin by your dermatologist can confirm whether or not a mole is dysplastic or atypical or is suspicious for malignant melanoma. If your dermatologist determines that a mole is suspicious for malignant melanoma then a biopsy will be performed. This is a simple procedure performed in the office under local anesthesia. Your mole will then be sent to a pathology lab where thin sections from the mole will be examined under a microscope by a dermatopathologist (a dermatologist or a pathologist trained in the microscopic examination of skin lesions). In the event your biopsy confirms a dysplastic mole or malignant melanoma, your dermatologist will discuss treatment options.
Individuals with dysplastic moles should have their skin inspected regularly by a dermatologist. In some cases, individuals should be inspected as frequently as every 3 months, beginning with the onset of puberty. Some dermatologists may also recommend regular ophthalmologic examinations and the use of digital medial photography to closely monitor some moles or areas of the body.
Inspection of your skin at home with a weekly skin self-exam can help you identify a suspicious mole and help your dermatologist diagnose malignant melanoma early. [Table 1]
When inspecting your skin for any moles, growths, or spots, look for these signs.
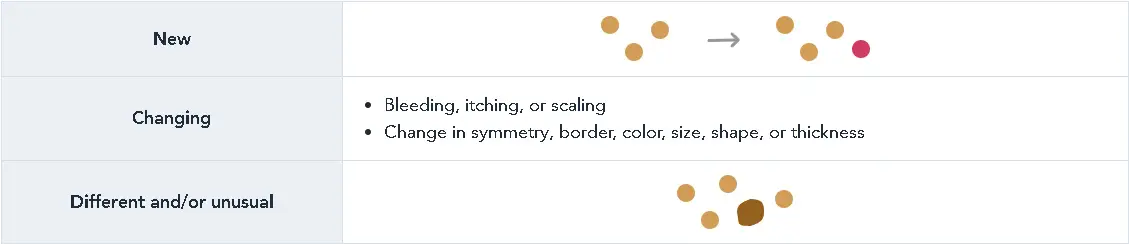
Table 01
Be suspicious of any new mole or growth, changing mole or growth, or mole or growth that looks different or unusual from those in the surrounding area. If any mole or growth is suspicious, you should immediately report it to your dermatologist as some aggressive types of malignant melanoma can spread inside your body within a few months.
When inspecting a single mole, only if you know it is a mole, it is helpful to apply the ABCDE rules to determine whether or not it is suspicious. [Table 2]

Table 02
Asymmetry: malignant melanoma has one half not matching the other half in size, shape, color, or thickness
Border irregularity: malignant melanoma has irregular edges that are notched, ragged, or scalloped
Color: malignant melanoma has a variety of colors within the same lesion, including shades of dark black and dark brown mixed with lighter tones; sometimes it may be red, pink, white, or skin colored
Diameter: malignant melanoma is larger than some surrounding moles, often greater than 6 millimeters or the size of a pencil eraser; however, malignant melanoma is less than 6 millimeters when it first appears
Evolving: malignant melanoma continues to grow and change, while other benign moles remain the same.
Treatment options
In the event your biopsy is diagnosed as a dysplastic mole and the entire mole was not removed, your dermatologist may schedule you for a conservative excision to completely remove the mole. For more information refer to “Common Procedures Performed in Dermatology”.
Follow-up care
Patients diagnosed with dysplastic moles should be examined by their dermatologist at least twice a year and sometimes up to four times a year. Remember, most individuals with a history of multiple dysplastic moles are more likely to develop malignant melanoma. Your dermatologist will inspect your skin for any new moles and will ensure that any previously treated moles are not growing back.
Patients with a previous history of dysplastic moles should also perform a weekly skin self-exam. Learning what malignant melanoma looks like may help you identify a suspicious mole earlier.
If you cannot see some part of your body, ask your partner or a family member to assist you with your weekly skin self-exam.
AVAILABLE ON




SkinIO HQ
171 N Aberdeen St. #400
Chicago, IL 60607
© Copyright 2025 SkinIO, Inc.